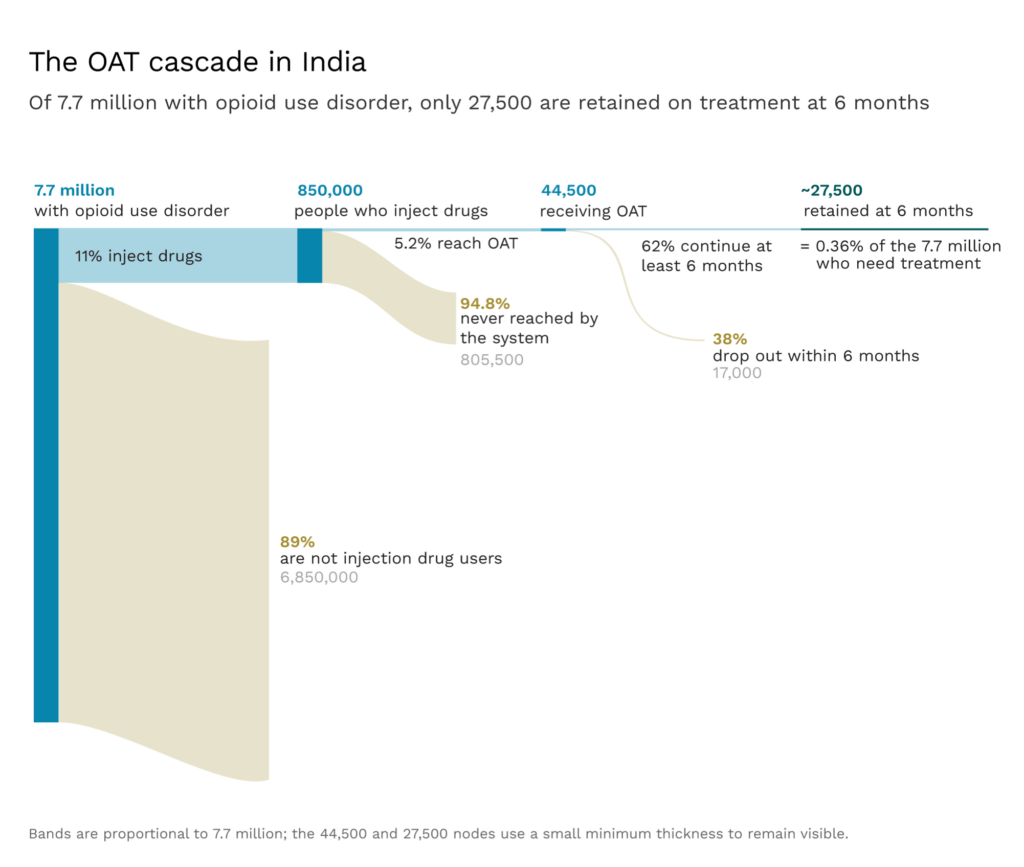
India produces enough buprenorphine, a medication used to treat opioid addiction, to serve about 450,000 patients each year. It is treating only 45,000. How do we fix this?
India has more people who misuse opioids than any other country in the world.1 But, of the 7.7 million people in the country who meet the criteria for opioid use disorders, fewer than 2% receive any evidence-based treatment.
Opioid addiction can sneak up on people. Many who use opioids don’t realize they’re dependent until they try to quit and then experience withdrawal. In Mizoram, one of India’s most afflicted states, the literal translation in Mizo for opioid-induced withdrawal symptoms is “suffer”. For users of opioids, “suffer” is as much a description as it is a metaphor. Coming off opioids involves severe cramps that seize the abdomen, sweating that won’t stop, tremors that look like convulsions, diarrhea and vomiting, chills, and many sleepless nights. Some of these symptoms can last for weeks.
Perhaps unsurprisingly, without sustained treatment, the rates of relapse among people who use opioids run between 80% and 90%. They then put off trying to quit again, because they simply don’t want to risk feeling that degree of pain a second time. But, after a relapse, the risk of fatal overdose is particularly high. While a user’s cravings may be just as intense, their body’s tolerance has decreased. Annual mortality among people who use opioids non-medically typically ranges from 1% to 3%.
Fortunately, for the last three-and-a-half decades, there has been access to successful treatment options. Opioid agonist therapy (OAT) recommends replacing illicit opioids with prescribed doses of methadone or buprenorphine. These opioid substitutes (agonists) bind to the same receptors in the brain, so they ease the cravings that users feel without producing the same “high”. This allows users to transition away from the dangerous parts of drug use without having to suffer withdrawal. This treatment works; these medications roughly double the likelihood of staying in treatment and cut the risk of dying from a drug overdose by about 70%.
Scaling OAT, then, seems like an obvious win. The therapy is relatively easy to administer—it can be done in an outpatient setting—and is very cheap. In India, the medication itself can cost as little as 25 to 30 US cents a day. The cost is clearly worth it; treatment pays for itself several times over because every dollar invested yields “a return of between $4 and $7 in reduced drug-related crime, criminal justice costs, and theft. When savings related to healthcare are included, total savings can exceed the costs [of OAT] by a ratio of 12 to 1.”2
And yet, OAT remains woefully underused in India. Just 2% of those who could benefit from it end up getting access, while the remaining 98% are left to fend for themselves. Other low- and middle-income countries manage to treat a considerably higher percentage of those who use opioids. If India scaled OAT to even 25% coverage—still below that of countries like Malaysia, Vietnam, and Iran—it could avert 5,000 to 7,000 deaths per year.3

Why is India failing on this issue?
It is not because policymakers think OAT doesn’t work. Instead, it is because three decades of policymaking have made it extraordinarily difficult to prescribe the medication, dispense it, or stay on it. India simply doesn’t trust its doctors or patients enough to implement international best practice.
Tracing the Boundaries of Opioid Use in India
Opioid use is not rare in India. About 2.1% of the Indian population uses opioids, roughly three times the world average. In any given year, about a third of those—or 7.7 million people—will engage in harmful opioid use. As a percentage of the population, opioid misuse is more common in India than in South Africa or Germany. And each year, at least 77,000 people will die from drug-related causes. This, too, is not a small number; it is similar to the number of Indians who die from breast cancer.
Injection drug users are the minority of Indian opioid users, making up only about 11% of those who misuse opioids.4 Most injection drug use in India is heroin, trafficked across borders from Myanmar. This means the epidemic is geographically concentrated in India’s northeastern states. Mizoram, Manipur, and Nagaland sit along trafficking routes from Myanmar, leaving them particularly exposed. Heroin also crosses from Afghanistan into Pakistan, and then into the street markets of India’s Punjab state.
The states of Mizoram, Nagaland, Arunachal Pradesh, Sikkim, and Manipur all have opioid use prevalence above 10% of the adult population. Between 4% and 7% of the population meet the criteria for problematic use; this is some 10 times the national average.

And in these places, the consequences of use extend well beyond addiction. HIV prevalence among people who inject drugs reaches 32% in Mizoram and 18% in Tripura. Hepatitis C prevalence exceeds 60% at multiple sites in these states. Getting the rules of treatment right here could reach a disproportionately large share of the national burden of infectious diseases.
The majority of users, though, smoke or take pills. Recently, India has seen the same expansion of pharmaceutical abuse that has been seen elsewhere in the world. India makes more generic drugs than any other country, and this includes opioid painkillers like tramadol and tapentadol, which are cheap and easy to get. Pharmacies routinely sell such drugs without a prescription. Indeed, the concept of prescription-only drugs is often more of a suggestion than a rule in many Indian pharmacies. This makes access easy and abuse more likely. About half of India’s opioid users now abuse via prescription drugs, rather than via heroin.
Getting Harm Reduction Right
To many, opioid agonist therapy does not seem like treatment at all. It sounds like simply providing drug addicts with their fix. Perhaps it is a less harmful way to take opioids, but they are still taking opioids. Is it really the role of the state to provide addicts with a different type of drug?
But to even ask the question is to misunderstand the treatment. Users on OAT do not get high, and they avoid the harmful parts of drug use. A major meta-analysis found that OAT reduces all-cause mortality by about a third to a half. It also reduces illicit opioid use, criminal activity, and the needle-sharing that spreads HIV. This is why OAT is the gold standard of treatment worldwide.
Over months and years, OAT allows people to lead stable lives in which they hold down jobs, save money, and rebuild relationships with their families. OAT treats opioid use disorder like any other chronic condition: the goal is not to get off the meds, but to have a functional, healthy life.
In rich countries, coverage is high. France treats more than 80% of its high-risk opioid users. Across the EU as a whole, roughly 60% of high-risk opioid users received OAT in 2023.
But it is not just rich countries that use OAT; it is also widely used in middle-income countries. For example, Iran began its national OAT rollout in the mid-2000s—about the same time India began scaling its program—and now delivers OAT treatment to 31% of those who would benefit from it. Vietnam’s treatment program reaches 25% of opioid users.5 India’s coverage rate is dismal by comparison: less than 2% of people in India who need it receive OAT.
How India Built The Wrong System
To understand why so many patients remain untreated, it helps to understand the history of OAT in India. Opioid agonist therapy was first introduced in India to counter the rise in HIV infections in people who injected opioids. HIV prevalence among people who inject drugs is more than thirty times the average prevalence.
OAT can help reduce these numbers. A patient stabilized on a daily oral dose of medication no longer feels the same degree of craving to inject other opioids, and the needle-sharing that drives infection stops.
So, the national scale-up of opioid agonist therapy began in 2007-08 through the National AIDS Control Programme. The goal was explicit: to reduce needle-sharing and HIV prevalence among those who inject opioids. At the time, this made sense; people who injected drugs made up a large and growing proportion of new HIV cases. India needed to reduce new HIV infections, and that meant OAT for injection drug users.
Even this was politically challenging. Since buprenorphine and methadone are opioids themselves, critics called the government an “official drug dealer.” In some ways, the government appeared to agree; the 2012 National Policy on Narcotic Drugs and Psychotropic Substances described OAT as treatment in which “an injecting drug user is supplied buprenorphine or methadone and persuaded to abuse them orally instead of injecting heroin or other drugs.”
The government treated OAT as if it were a stop on the way to recovery—a slightly shameful stop at that. The policy went on to impose a one- to two-year cap on agonist treatment, insisting that patients be switched to “de-addiction as soon as possible preferably within one year but in no case later than two years.”
There is no scientific basis for this time limit. Opioid dependence changes brain chemistry in ways that take many years to reverse, not just one or two. A recent cohort study of 32,000 US veterans that tracked treatment durations of up to six years found that survival kept improving with each additional year on treatment, and that the commonly recommended six-month minimum was “likely insufficient, regardless of the patient’s individual mortality risk.”
As one review put it, the question isn’t how to get patients off medication; it’s why we’d want to when they’re already doing well on it. This is why the WHO, since 2009, has recommended that “in most cases, treatment will be required in the long term or even throughout life,” and that this “should not be seen as a failure, but rather as a cost-effective way of prolonging and improving the quality of life.”
And yet, as recently as 2022, newspaper articles ran with headlines like “Punjab’s OOAT6 plan goes awry, addicts get hooked on treatment pills!” In 2023, Punjab’s health minister complained that despite improving access to medications, there weren’t enough patients who had been “cured” of opioid use disorder. But this is a fundamental misunderstanding of opioid use disorders. It is like asking for a cure for diabetes or hypertension. For opioid use disorder, cure is possible, but unlikely; consistent, managed treatment works for nearly all patients.
Embedding OAT within the HIV program was, in part, a way to borrow the institutional legitimacy and international funding that HIV treatment provided. This was a pragmatic choice; few would argue against reducing HIV infections. But there were significant tradeoffs. Because OAT was built as an HIV prevention tool, the program of the National AIDS Control Organisation (NACO) only registers patients who inject drugs. But this leaves out almost 90% of those who could benefit from OAT. The other 7 million people smoke or “chase” heroin, drink opioid concoctions, or take pills — and they can’t access NACO-affiliated treatment centers.
Where do non-injecting opioid users go instead? Government de-addiction centers offer short-term inpatient detoxification: patients are stabilized, withdrawn from opioids over days or weeks, and then discharged. But relapse rates after opioid detoxification are as high as 90%, with most patients relapsing within weeks of discharge. This is because detoxification only clears the drug from the body. It doesn’t undo what months or years of opioid use have done to the brain. Long after withdrawal, cravings persist, the ability to feel normal pleasure doesn’t return immediately, and the body continues to be sensitive to stress.
Worse still, patients are at high risk of overdose after detox. During detox, opioid tolerance drops sharply. When patients relapse, and most do, they return to doses their bodies can no longer handle.
Recently, India has begun to include non-injection opioid users in their treatment plans. Drug treatment clinics have been set up in government hospitals to provide OAT to anyone with opioid use disorder, not only those who inject. But by 2019, there were only 27 such clinics across the whole country. Clearly, this does not suffice to serve 7 million patients.
Punjab is the one place in India where this approach has been scaled.7 Government-run outpatient clinics now accept any opioid-dependent patient regardless of injection status.
Evidence-Based Policymaking
There is another significant problem. Indian policymakers haven’t faced the scale of the crisis. The government’s programmatic mapping exercise, conducted between 2020 and 2022, estimated there were about 289,000 injection drug users in India. But the Magnitude of Substance Use in India study, conducted by the All India Institute of Medical Sciences (AIIMS) and the Ministry of Social Justice and Empowerment in 2018 put the number at about 850,000. The latter number is likely more accurate as it is designed to capture hidden populations away from obvious hotspots.
Different parts of the Indian government use each figure; the Narcotics Control Bureau has since adopted the higher figure, but the National AIDS Control Organisation, which runs the OAT programs, uses the lower one. Planning for the lower number will leave half a million injection drug users out in the cold, and it certainly leaves no spare capacity to reach other types of opioid users.
Even if there were only 289,000 opioid users, India simply doesn’t have the clinics it needs. In the decade to 2023, the country went from essentially zero national OAT coverage to 393 centers. Punjab has added a further 529 clinics. But just short of a thousand clinics can hardly cover 7 million people across 28 states.
The situation for women is particularly bleak. Women who undergo treatment in women-only centers show less substance use and criminal activity compared to those in mixed-gender programs, but there are only four women-only drug de-addiction centers in the entire country.
There are viable solutions to this dearth of treatment facilities. If community health centers and primary care physicians could prescribe and dispense OAT, the number of access points would increase dramatically without the need to create new centers. As of 2023, India already had over 30,000 primary health centers and about 170,000 sub-centers. Even a small fraction of these offering OAT would radically increase coverage.8
Beyond Government Clinics
In a country the size of India, though, government-affiliated clinics probably won’t be enough. Private providers can help fill this gap. This is relatively common across countries that provide OAT; Iran, for instance, has more than 7,000 private outpatient clinics dispensing OAT.
In principle, Indian psychiatrists could follow Iran’s example. There are private de-addiction centers in India, and private psychiatrists are legally permitted to prescribe buprenorphine. In practice, very few facilities offer OAT because private psychiatrists simply don’t want to take the risk.
Prescribing buprenorphine is a regulatory grey zone, with conflicting directives. Buprenorphine is simultaneously regulated under four different legal instruments: the Narcotic Drugs and Psychotropic Substances Act 1985, the Drugs and Cosmetics Act 1940, the Mental Healthcare Act 2017, and separate Drug Controller General of India approval conditions, and none of these agree on who can stock, dispense, or prescribe the drug. In the past, psychiatrists have been arrested for providing buprenorphine without the right licenses.
Consider (again) the example of Punjab. While it has had success in expanding government-affiliated clinics, private clinic expansion has not gone so well. In 2019, the Drug Controller General of India issued a directive that private psychiatrists could dispense buprenorphine from their own clinics. But, before the rules could take effect, the Punjab and Haryana High Court stayed the change. In 2020, the state’s cabinet amended its rules to allow private clinics to dispense anyway, but, by 2021, that provision had been rescinded. Four years later, in June 2025, citing the shortage in the public system, the Punjab health minister announced that private psychiatrists would be allowed to dispense in their outpatient departments. But, within weeks, the 2019 stay resurfaced as a legal barrier, and the health department set up a committee to decide how to get it vacated. In October 2025, the state cabinet issued new rules that specifically allowed individual psychiatrists to provide OAT without running a full inpatient rehab, but, within weeks, a public interest petition was filed challenging the rules. The petitioner argued the outpatient-only category was inconsistent with the Mental Healthcare Act and would encourage unregulated dispensing and diversion. At the time of writing, the matter was pending before the Punjab and Haryana High Court.
Unsurprisingly, all this flip-flopping has put private practitioners off OAT entirely. No official count of private facilities has ever been published, but the number appears negligible. In India, prescribing OAT may be harder than prescribing the opioid itself.
A Dosage That Causes Suffering
Even if a patient can reach one of the few government-affiliated clinics, the current system makes it difficult for them to stay in treatment. For a start, clinics radically underdose patients.
India’s early experiments with buprenorphine in the 1990s used very low doses of 1.2 to 2 mg per day, in part because only 0.2 mg tablets were available at the time. After larger doses became available in the 2000s, a very small-scale local study in India compared the efficacy of 2 mg and 4 mg doses. It showed no difference in efficacy, likely because the study only had 23 patients. Indian policymakers stuck with the lower, cheaper dose.
Unfortunately, early studies were misleading. The WHO now recommends 8 mg to 24 mg per day for buprenorphine maintenance. At lower doses, patients are much more likely to still experience withdrawal and cravings. Since patients still suffer the negative side effects of coming off drugs, they are much more likely to discontinue treatment. A meta-analysis found that patients on 16 mg or more stayed in treatment longer and tested clean more often than those on lower doses.
India has since updated its guidelines somewhat, but they remain far below international norms. More than three-quarters of patients at government-affiliated treatment centers were receiving less than 8 mg daily and, as a consequence, about 38% had dropped out by six months. There has been no attempt to see whether higher doses could reduce this dismal retention rate.
Increasing the dosage received at clinics to the WHO standard would not require major changes. Since dosing is centralized in a relatively small number of clinics, it would be relatively simple to require these government-affiliated clinics to provide at least 16 mg of buprenorphine daily in consultation with the patient. Since buprenorphine is so cheap, it would not even be a major strain on government budgets.
Barriers to Staying in Treatment
But let us say a patient can get to a clinic and tolerate the ongoing cravings. India’s clinics still make it difficult to stay in treatment. Indeed, they give patients a seemingly never-ending series of obstacles.
When a patient starts OAT, the consent form requires a family member or witness to co-sign, and patients must agree to bring family along for follow-up visits. At many centers, this means a patient cannot begin treatment without first disclosing their addiction to a relative. Given the severe stigma of opioid addiction, that is not a small ask.
The family obligation doesn’t stop at registration. On weekends, when clinics are closed, a family member must collect the patient’s doses and supervise them at home. The patient cannot take the medication unattended. The logic behind this is that families support recovery and that involving them early builds a structure around the patient. But not everyone has a willing family member, particularly if they have struggled with opioid addiction that has strained family relationships.
The logistical difficulties do not end there. In India, OAT requires daily attendance at a clinic. Medication is given as a small tablet, often crushed and placed under the tongue. Staff watch it dissolve so it can’t be pocketed and carried out. But most clinics are only open from 9 am to 4 pm. When travel to and from a clinic is included, treatment can take hours a day, and most of those hours must be during the workday. In a country where many laborers work in informal jobs without the ability to even discuss taking time off, it can seem easier to discontinue treatment than to try to manage the logistics.
Seasonal migration makes these constraints even harder to navigate. In India, it is estimated that between 2% and 6.8% of people migrate seasonally. But when clinics require frequent in-person attendance, OAT becomes difficult to sustain. In a set of interviews with young people who inject drugs in the northeast state of Mizoram, one patient described the problem:
“We went to my wife’s village. We expected the length of our stay to be one week, one week and a bit. But they could not give us too many OATs. Maybe it was two or three days’ dose; they gave us just that. During that time, if I didn’t take it, I still had to suffer.”
So, people adapt. For travel, they borrow doses from others at the clinic, then smuggle out their own daily allotment after they return to repay the loan. In Punjab, researchers have documented this barter system among truck drivers whose trips can last a month. Most of the “diverted” buprenorphine is probably consumed by people already in treatment, not by new users chasing a high.
In many countries, take-home OAT is much more common because they have adopted an important technological improvement. Rather than using just buprenorphine, they use buprenorphine combined with naloxone. In this formulation, an opioid-like molecule, buprenorphine, and its antagonist, naloxone, are combined. When you swallow the tablet, naloxone is poorly absorbed and has little or no effect, while the buprenorphine works as expected. But if someone dissolves and injects the tablet to get high, the naloxone blocks the opioid receptors and triggers withdrawal symptoms. This means it is safe for take-home dosing since the patient can’t get high on it even if they try.
The combination works well elsewhere. In the United States, buprenorphine is prescribed like any other Schedule III medication, with patients receiving up to a month’s supply at a time. The longer patients stay on treatment, the better the outcomes. We know that the combination product—buprenorphine mixed with naloxone—is as effective as buprenorphine alone, suppressing withdrawal and cravings.
While there have been concerns that the effects of naloxone may be too short-lived to prevent diversion in all forms, there is some concrete evidence that its design to deter abuse works. Patients prescribed buprenorphine-naloxone consistently report injecting it for misuse less often than those on plain buprenorphine. Weekly injection rates in Australia ran roughly half those of buprenorphine alone, daily injection rates among Finnish needle-exchange participants about a fifth, and US surveillance data show a similar gap.
This combination does exist in India. The buprenorphine-naloxone combination was launched in the country in 2004-2005. It is not clear why it hasn’t become the standard medication of choice for take-home dosing.9
But during the COVID-19 pandemic, India experimented with longer dosing. NACO allowed take-home buprenorphine for the first time, with centers dispensing at least seven days’ supply, and even up to four weeks’ provision in some tertiary centers. A retrospective cohort study at one North Indian tertiary center compared patients given a 1- to 2-week supply before the pandemic with a cohort given up to 4 weeks during it. The longer-prescription group stayed in treatment longer.
But even the combination therapy is just a better version of the same daily pill. The science has moved further along. In April 2026, the WHO added long-acting injectable buprenorphine to its treatment guidelines, recognizing that a monthly injection eliminates the need for daily clinic visits that drive patients out of treatment, and removes the diversion risk that drives daily dispensing recommendations. And even better options are on the horizon: subdermal implants could offer six months of steady medication from a single procedure, and early research on GLP-110 receptor agonists like semaglutide suggests they may reduce opioid cravings. Trials are in progress in the US right now, but there are no such trials in India. India must move beyond 1990s science and find the best ways to treat its large opioid-dependent population.
Fixing the Problem
It is not that India lacks the medicine or the money to treat opioid addiction. Rather, it is that the country’s opioid treatment system was built on a deep mistrust of the people within it. Patients are treated like addicts without the willpower to get clean, not as people dealing with a physiological dependence. Every choice in the system underlines that reducing the risk of misuse outweighs any suffering patients may experience along the way.
Most of these choices can be unwound, and most without much money. India can plan for all those who are dependent on opioids, not just the ones the government deems acceptable to count; raise government clinic dosing to the WHO range; make buprenorphine-naloxone the default take-home medication; and let primary health centers and private clinics prescribe and dispense without putting themselves in legal jeopardy.
None of these require inventing anything. The evidence base is decades old, the international playbook has been successfully followed in many other countries, and India is well-placed to implement a better system. Indian patients should not need to suffer any longer.
Akshay Narayanan is a public health researcher and consultant working on treatment for young people with opioid use disorders in India and violence prevention in schools across low- and middle-income countries. He previously led child protection programs for Guardians of Dreams, and writes about how young people shape the world and how the world shapes their lives.
If you have comments on this article, or wish to contribute to the discussion, please email them to letters@indevelopmentmag.com. Responses will be featured in a letters section.
- As calculated from prevalence numbers from the World Drug Report 2025. Some sources have the US as having a slightly higher number of people with opioid use disorder; given the difficulty surveying this population, there is some variation among sources. ↩︎
- This cost-effectiveness estimate is from the US; no similar estimate exists in the South Asian context, despite nearly two decades of OAT delivery in India. ↩︎
- India’s National Crime Records Bureau reported about 3,000 drug-related deaths between 2019 and 2023 but this figure is universally regarded as a severe undercount. As Singh and Rao (2012) note, opioid overdose deaths in India are routinely registered as “cause unknown” or as exposure to cold or heat, particularly among the homeless. The figure also captures only “accidental” opioid overdose. It excludes the far larger toll of drug-attributable mortality from HIV and Hepatitis C transmission through shared needles, injection-related infections, and mental health comorbidities. The true baseline against which any treatment scale-up would operate is almost certainly an order of magnitude higher than the official count.
Scaling OAT from 2% to 25% would put an additional approximately 1.77 million Indians into treatment. Of those, baseline annual mortality would be about 18,000 to 27,000. Applying Sordo’s 55% reduction in all-cause mortality only to the fraction meaningfully retained in treatment (assume even half, given conservative retention rates) yields roughly 4,900 to 7,300 lives saved per year from mortality reduction alone. ↩︎ - Some heroin users inject, although in India it is more common for heroin to be smoked. ↩︎
- As of December 2022, Vietnam had 235,314 registered drug users, of whom 84.7% use opioids. There are 52,000 people in treatment, which is about 25%. ↩︎
- Outpatient Opioid Assisted Treatment. ↩︎
- There are now 529 such clinics in Punjab. ↩︎
- Indeed, this is precisely how Punjab has been expanding access to OAT to address its growing opioid crisis. ↩︎
- Perhaps it is because the NACO guidelines reference only plain buprenorphine. Given the legal uncertainties, it does not make sense for prescribers to push for something not explicitly covered by regulation. ↩︎
- Glucagon-like peptide-1 ↩︎